🌟 Marvix is exhibiting at the Thrive Summit 2025 by athenahealth | Nov 3-5 | Nashville, TN | Come visit us at our booth 👋
🌟 Meet Marvix at the 2025 AAN Fall Conference | Nov 7-9 | Las Vegas | Stop by our booth 😊
🌟 Marvix joins the stage at the WHCMAA Alumni Conference | Nov 13-14 | Philadelphia, PA | Catch our panel discussion 🎤
🌟 Marvix is exhibiting at McKesson Accelerate 2025 | Nov 3-5 | Wynn Las Vegas | Meet us at our booth 🎤
The Invisible Tax on Specialty Medicine
Marvix Editorial Team
July 3, 2025
•
6 min read
Clinical documentation in specialty care is anything but straightforward. Specialty workflows demand the integration of data scattered across time, teams, and systems. A single consult note might require pulling in information from physician and patient conversations, care team discussions, intake forms completed by medical assistants, past treatment summaries, chronic condition notes, lab and diagnostic reports from outside institutions, and a mix of faxes, transcripts, and handwritten paper notes.
This data lives in silos—across current and prior EHRs, scanned paper documents, dictation audio files, and in the minds of multiple people involved in the patient’s care, including the patient and their caregivers. The complexity compounds over time: a comprehensive treatment summary for a cancer patient, for example, may require stitching together three years of fragmented documentation from multiple institutions and sources.
The Status Quo: Brute Force and Burnout
Today, this problem is being solved with brute force. AI meeting summarizers capture only a sliver—maybe 2%—of what’s truly needed to generate a complete, accurate clinical note. The heavy lifting still falls on the shoulders of human teams: physicians, medical assistants, and nurses who spend hours combing through PDFs, printing and annotating faxes, retyping data into EHRs, and manually writing summaries.
This problem is far from solved. Manual charting still dominates because data is scattered across disconnected EHR modules, scanned PDFs, faxed labs, and outdated templates. Clinicians waste valuable time hunting for information—clicking through medication tabs, reviewing irrelevant problem lists, retyping histories that already exist elsewhere. It’s not just inefficient—it’s administrative overload disguised as clinical work.
The result? Massive physician burnout, lost productivity across care teams, suboptimal patient care because providers are just focused on documentation—and critical clinical details falling through the cracks.
Moreover, about 70 percent (Miller Wagner) of patient records have incorrect or missing information, which can lead to adverse or even fatal outcomes, including misdiagnosis, inappropriate medication, and missed allergies. So how do we solve this?
Why Most AI Scribes Fall Short
Most AI scribes fail in specialty care because they only summarize the current conversation. But clinical documentation isn’t just about what was said—it’s about connecting that moment to everything that came before. Meeting-style summaries miss the mark.
Specialists don’t need transcripts. They need notes that reflect their thinking, history of the patient’s condition(s), and treatment strategy—grounded in that point in time within the patient’s overall care journey. These traditional AI scribe notes are at best incomplete or at worst highly misleading.
Marvix AI: Built for the Real Work of Specialty Care
At Marvix AI, we intend to change that. We’ve built a purpose-built workflow engine that doesn’t just listen to conversations—it consolidates, contextualizes, and connects data across all touchpoints to generate a complete, clinically meaningful note that integrates directly into the EHR and supports true continuity of care.
Let’s dig deeper into how we solve this.
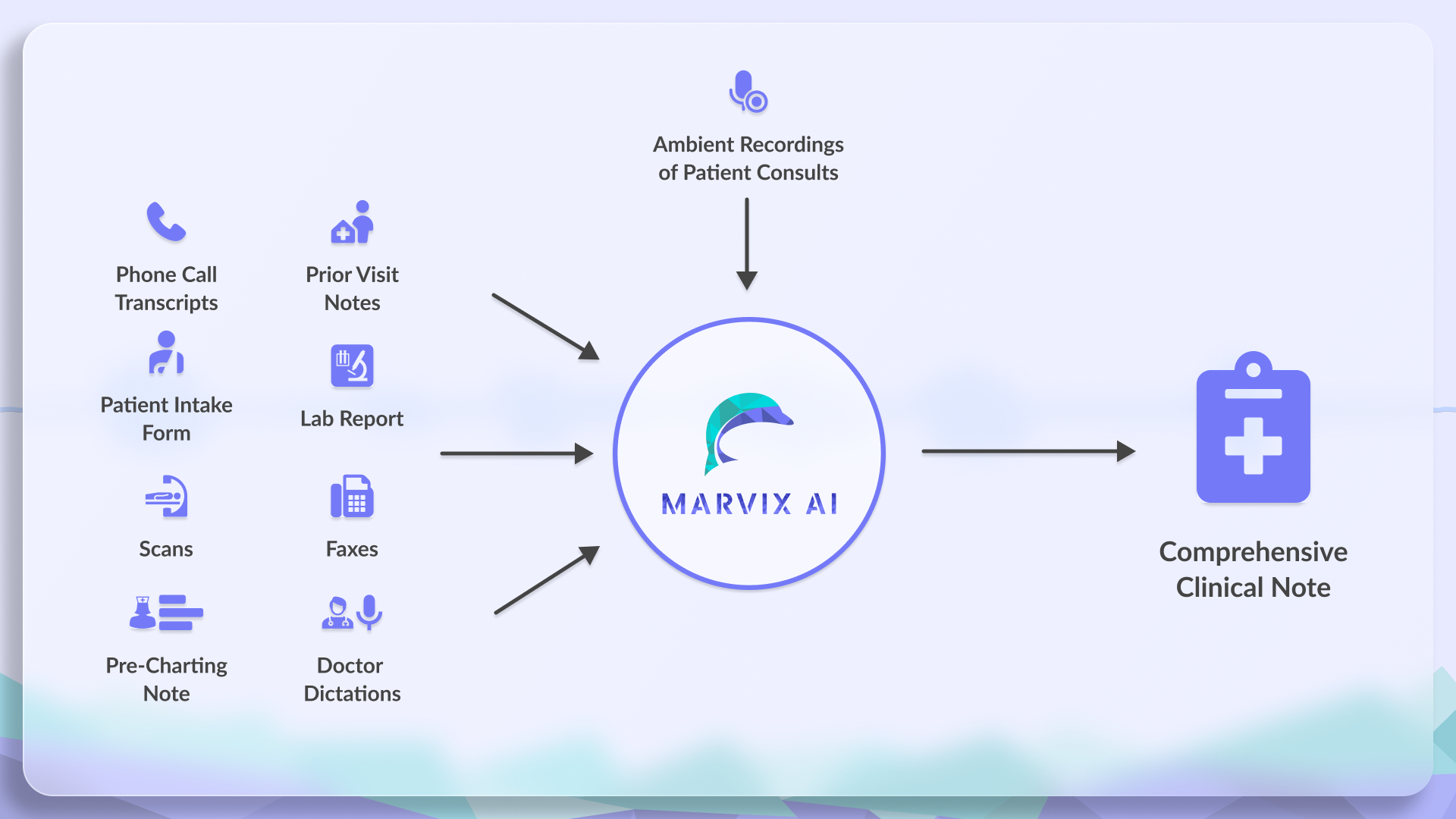
Step 1: Ingesting All the Right Information
Marvix seamlessly integrates diverse clinical data—from previous notes and external consults to imaging reports and dictations—pulling structured insights from multiple formats and sources.
Marvix directly integrates all the necessary information into the note. It pulls structured data from the following critical sources.
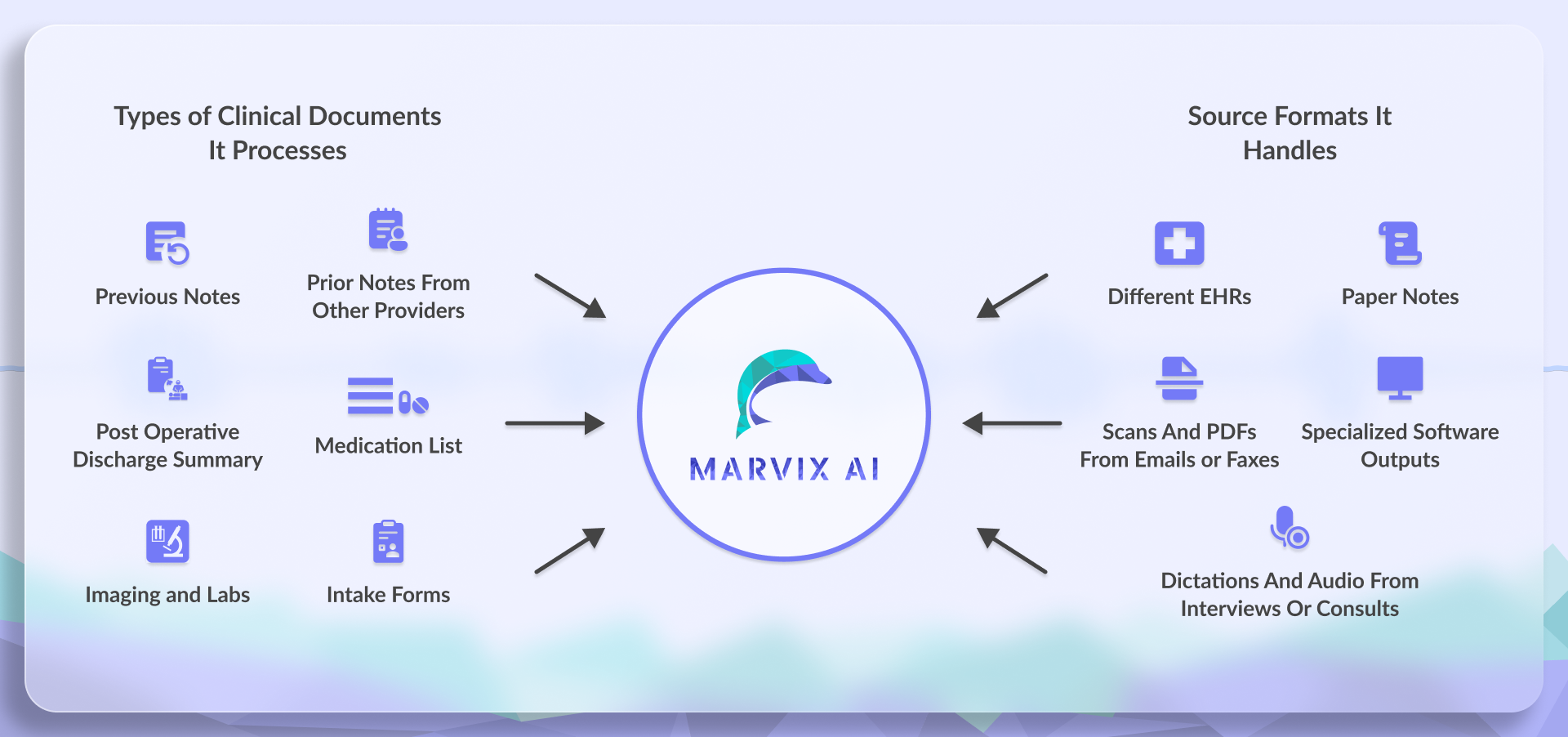
Types of Clinical Documents It Processes:
Previous notes: Extracts assessments, clinical impressions, and unresolved problems from past documentation. It also carries forward all current diagnoses.
Prior notes from other providers: Captures handoffs, second opinions, and external consult notes across care teams.
Post-operative discharge summaries: Surfaces key details like surgical outcomes, instructions, and pending follow-ups.
Medication lists: Retrieves active and historical medications, including dosage changes, tapers, and discontinued drugs.
Imaging and labs: Pulls forward reports, summarizes findings, and lab results ordered in earlier visits.
Intake forms: Ingests structured or unstructured intake documents—including scanned PDFs and paper questionnaires—with symptom scales and patient-reported concerns.
Source Formats It Handles:
Different EHRs: Pulls structured data across multiple EHR systems, regardless of format or vendor.
Paper notes: Digitizes and extracts relevant information from handwritten or printed clinical notes.
Scans and PDFs from emails or faxes: Ingests scanned documents, attachments, and faxed files—no need for manual uploads.
Specialized software outputs: Parses complex formats (like DICOM images from radiology software) and integrates findings directly into the note.
Dictations and audio from interviews or consults: Transcribes and extracts insights from recorded clinician-patient conversations.
Step 2: Making Sense of Fragmented Medical Data
Marvix converts scattered, inconsistent patient data across EHRs, scanned forms, PDFs, and legacy reports into one clean, structured clinical snapshot.
In specialty care, past data isn’t just scattered—it’s fragmented across incompatible formats, legacy systems, and disconnected institutions. Prior notes may originate from different EHRs entirely, often delivered in CCDAs or non-standardized text exports. Lab reports might come from external facilities with proprietary templates. Intake forms could be scanned paper documents, flattened PDFs, or free-text submissions. Medications may be listed in outdated, partial formats depending on the prescribing system.
Even when old data is accessible, it’s rarely consistent—formats vary, naming conventions differ, and clinically relevant sections are buried across multiple documents.
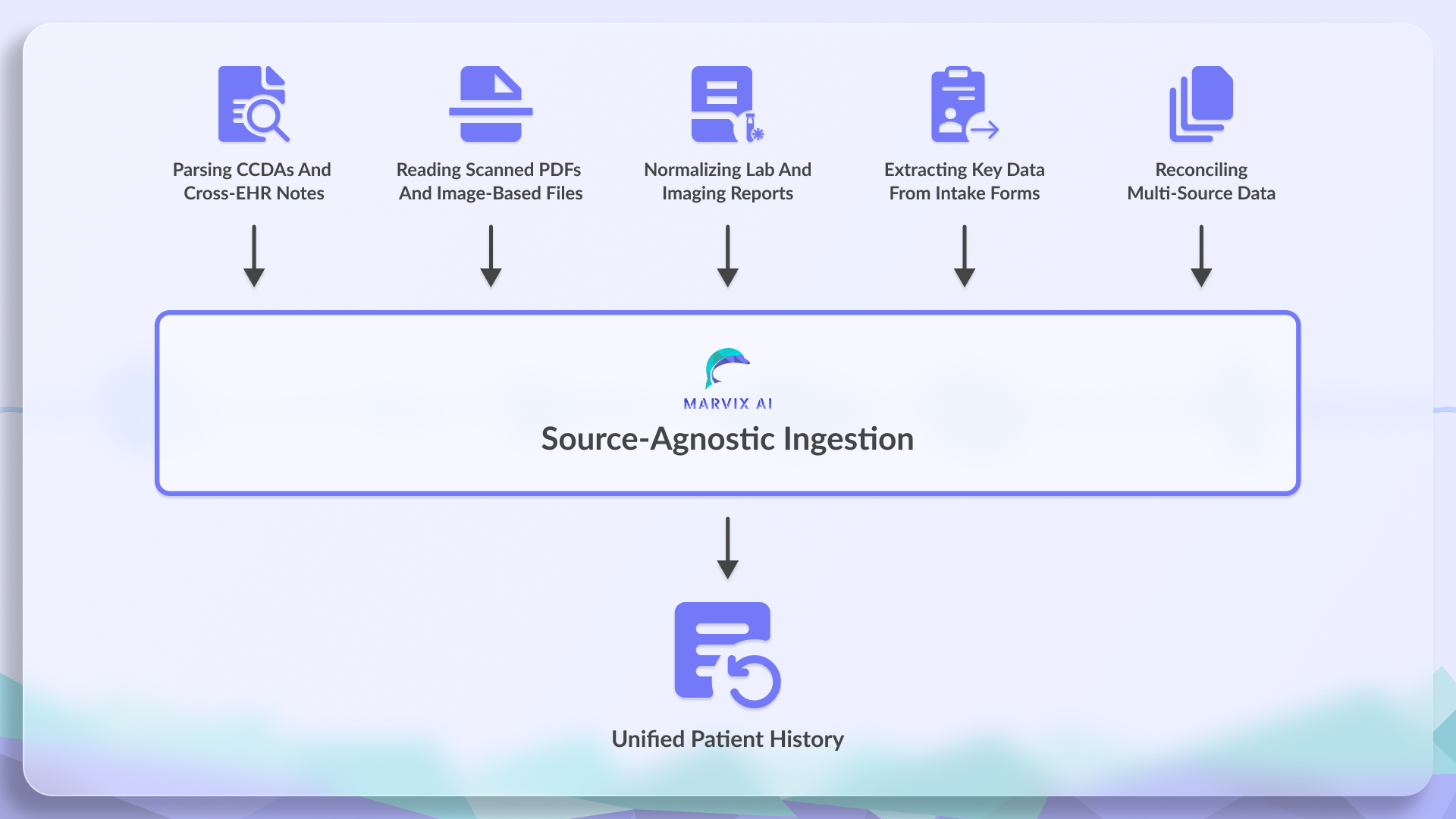
Marvix processes this fragmented data and converts it into a usable clinical layer by:
Parsing CCDAs and cross-EHR notes to extract relevant clinical sections while filtering out noise.
Reading scanned PDFs and image-based files using document-level OCR and semantic segmentation.
Normalizing lab and imaging reports from non-standard sources by mapping fields into structured, codified entries.
Extracting key data from intake forms, whether typed, scanned, or handwritten, using intelligent form detection.
Reconciling multi-source data across systems and formats into a single, structured input for note generation.
This allows Marvix to build a clean, unified view of the patient’s past—regardless of where the data came from or how it was originally formatted.
Step 3: Handling Data Protocol Chaos at Scale
Marvix’s multi-format ingestion engine decodes complex healthcare protocols—FHIR, HL7, proprietary APIs, scanned docs—and normalizes them for unified, reliable documentation.
The complexity of medical data isn’t just about content—it’s about the formats and protocols that deliver it. Clinical information comes from dozens of sources: EHRs, labs, imaging centers, outside providers, and internal systems. Each uses its own data format, structure, and delivery mechanism. Even when the data is available, accessing it isn’t straightforward.
Some systems expose FHIR APIs, which are structured but often incomplete or inconsistently implemented.
Others rely on proprietary APIs, requiring custom integrations and ongoing maintenance.
Legacy systems may still use HL7 v2 messages, a format designed decades ago, often undocumented or poorly mapped.
Scanned documents, PDFs, and CCDAs add yet another layer of incompatibility—requiring parsing, normalization, and error handling.
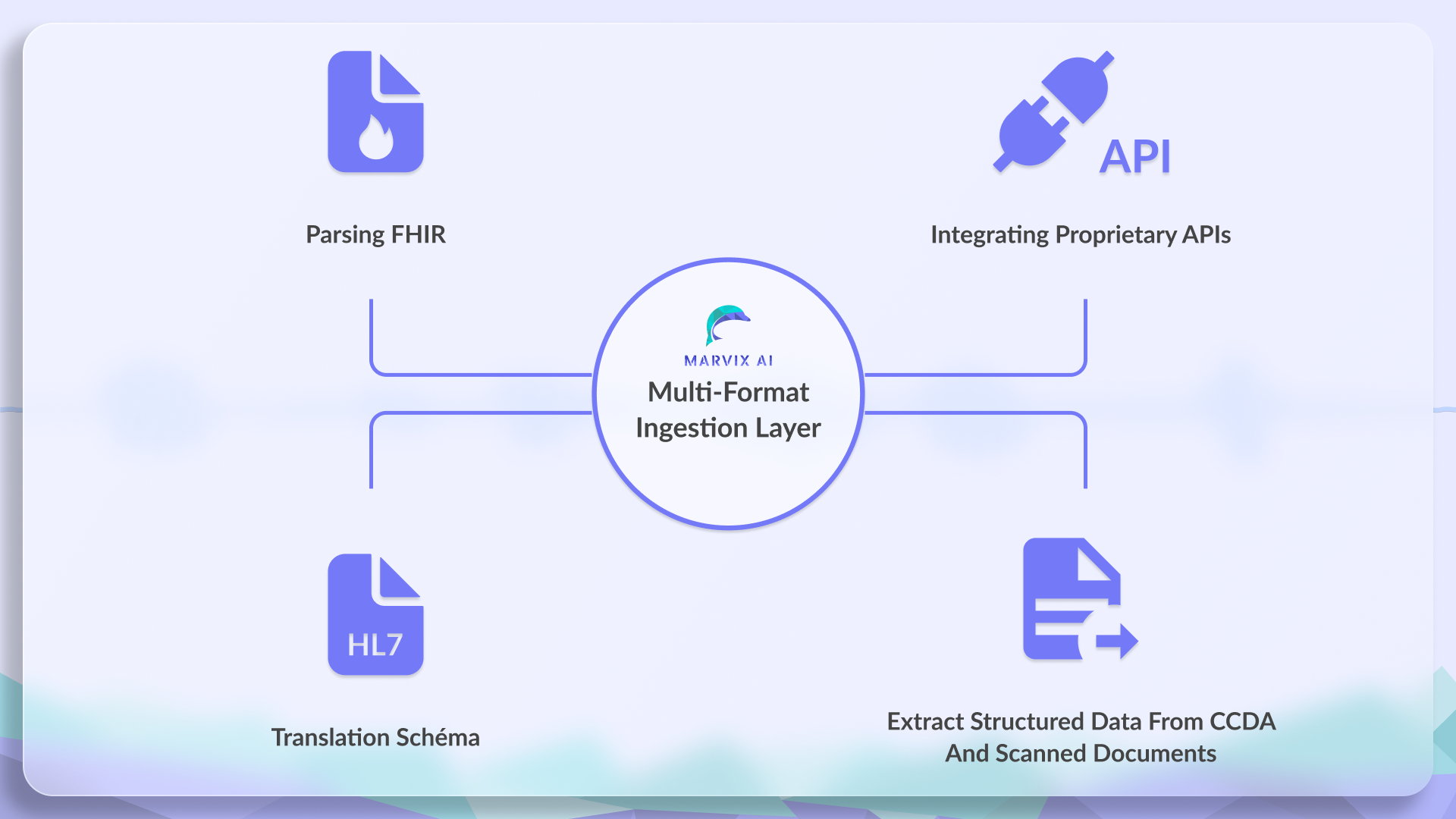
Marvix handles this heterogeneity by building a multi-format ingestion layer:
Parses FHIR when available
Integrates proprietary APIs using system-specific connectors
Decodes HL7 messages with schema translation
Extracts structured data from CCDAs and scanned documents using large language models
No matter the source or format, the output is normalized and structured—ready to drive clinical documentation downstream.
This multi-format ingestion pipeline allows Marvix to pull clinical data from virtually any system and normalize it—regardless of the underlying standard or delivery method.
The Result: A Real Clinical Note, Not a Meeting Recap
By combining all of this upstream information, Marvix produces documentation that reflects a patient’s true clinical journey and not just what is discussed in the present day consult with the doctor. 0% data loss, 100% medical accuracy.
Moreover, this entire process is automatic! We extract your documents in all formats from your EHR, you can upload additional files on Marvix—we summarize everything in the back end, capture your present-day interactions ambiently and create a finished, consolidated clinical note in just a few minutes.
Marvix is your super-intelligent clinical assistant that never tires and operates at supersonic speed. :)
Real-World Case Studies in Specialty Care that Marvix handles
Case Study: Oncology
A 62-year-old woman returns to her oncologist for a follow-up visit. She was first diagnosed with stage III colon cancer three years ago. Since then, her care history has spanned:
A surgical resection captured in an inpatient discharge summary
Six rounds of adjuvant chemotherapy documented across infusion clinic notes over multiple months.
Imaging that revealed hepatic metastasis, captured in a radiology report from an external facility
A second-line chemotherapy plan created during a multi-specialty tumor board discussion, summarized in a scanned PDF
Ongoing labs tracking CEA levels, scattered across multiple outpatient visits
A recent medication change initiated by another oncologist she saw while temporarily out of town
Symptom questionnaires submitted by the patient on paper during each chemo infusion visit.
By the time she’s back in clinic today, her current oncologist has to reconstruct this longitudinal history from:
Two different EHR systems
A faxed consult note
A CD-ROM radiology report scanned into the system
Paper intake forms
A CCDA from her recent out-of-network provider
Her last progress note from 7 months ago
This isn’t uncommon. The clinical reality in oncology often spans years, institutions, formats, and fragmented inputs.
How Marvix handles it: Marvix ingests all of these inputs—across EHRs, PDFs, CCDAs, scanned imaging summaries, and handwritten forms. It parses the relevant clinical signals, recognizes unresolved problems, tracks treatment milestones, reconciles medication changes, and brings forward the right labs and imaging summaries.
The resulting note isn’t just a visit recap—it’s a clinically informed summary that carries the patient’s entire trajectory forward.
In addition, Marvix ambiently records her present day consult with her oncologist and creates a clinical note that is informed by the transcript of the current consult as well as her longitudinal summary that was created from all the different reports over the last 3 years.
The result is a well informed clinical document that allows her oncologist to recommend the right course of treatment knowing fully well her medical history. Moreover this document is insurance ready as it checks all boxes on prior history documentation requirements.
Case Study: Neurology
A 37-year-old man with a history of traumatic brain injury presents for evaluation. Three weeks ago, he was involved in a motorcycle accident. His initial care included:
An ER visit with imaging, labs, and a full discharge summary
A CT scan that revealed a small subdural hematoma
A neuro consult during inpatient stay, documented in a separate EHR
Follow-up MRIs conducted at an outpatient radiology center
Audiology and vestibular tests run at a balance clinic
A paper symptom scale filled by the patient’s spouse tracking mood and cognitive changes
A medication list altered twice—once by the ER, once by his primary care doctor
His neurologist now needs to:
Understand the sequence of events since the accident
Review radiology and balance testing results
Compare medication adjustments over time
Incorporate behavioral changes noted by the caregiver
Plan a long-term rehabilitation strategy
But the data sits in:
HL7 ER messages
Scanned PDFs from outpatient imaging
Free-text email summaries forwarded from other providers
Printed paper test results
Dictated audio files from his neuro consult
Disparate EHRs from hospital and outpatient care
How Marvix handles it: Marvix pulls and parses all of this—decoding HL7 messages, reading and summarizing PDFs, extracting meaning from audio consults creating digital summaries, and making structured sense of balance tests and medication shifts. It creates a complete neurological note that accounts for the patient’s post-trauma arc and supports informed planning.
Instead of manually stitching together fragments, the neurologist gets a note that reflects clinical continuity and an exhaustive summary of the patient’s entire clinical history till date.
This informs his decisions on medical management for the present day consult and results in saving at least 4 hours of time that the provider or his medical assistant would have spent in creating this history.
More Than Notes. Marvix Thinks Like You Do.
Specialty care runs on context—yet clinical documentation remains stuck in fragments. Physicians waste hours stitching together data from EHRs, faxes, scans, and handwritten notes, while critical details slip through the cracks. The cost? Burnout, errors, and patient care compromised by administrative chaos.
This isn’t a problem point solutions summaring current consults can solve. Real documentation requires continuity—connecting today’s decisions to everything that came before.
Marvix AI was built for that work. We ingest data from every source, in any format, and structure it into notes that reflect how specialists think: complete, clinically relevant, and grounded in the patient’s full history.
The result: clarity and more focus on what matters. Because when documentation finally keeps up with medicine’s complexity, care improves. For physicians. For teams. For patients.
The tools exist. The time is now. Let’s build a process that works. We are here to help!
Unsure on how Marvix can solve your unique workflow requirements? Book a demo here and get a 30-day complimentary trial.


.png)